MedTech Intelligence – Read More
Introduction: PMS Is Working—But Not Where It Matters Most
Post-market surveillance (PMS) systems across the medical device industry have never been more mature. Organizations are capturing complaints, monitoring adverse events, generating Periodic Safety Update Reports (PSURs), and meeting increasingly complex global regulatory requirements.¹⁻⁴
From a compliance standpoint, PMS is working. But from a clinical and patient-impact perspective, a critical gap remains; organizations are collecting more data than ever without consistently translating it into timely, actionable clinical decisions.
Large global MedTech organizations frequently process substantial complaint volumes annually, alongside hundreds of trend analyses and statistical alerts across products, regions, and failure modes. Yet only a small percentage of these signals ultimately require meaningful escalation such as CAPAs, Health Risk Assessments, or Field Safety Corrective Actions.
The challenge is no longer simply detecting signals. It is determining which signals truly matter, how quickly they require action, and how effectively insights are translated back to clinicians and patients. As devices become more software-driven, connected, and data-intensive, organizations can no longer rely on retrospective reporting models alone. Modern PMS systems must evolve into operational decision-support systems capable of enabling proactive risk management and timely clinical response.
At the same time, clinicians and healthcare systems are increasingly overwhelmed by information overload. Static reports and retrospective summaries may satisfy documentation expectations, but they rarely provide actionable insight at the point of care. The organizations that succeed in the next phase of MedTech will be those capable of translating complex post-market data into meaningful clinical and operational decisions.
The Broken Feedback Loop
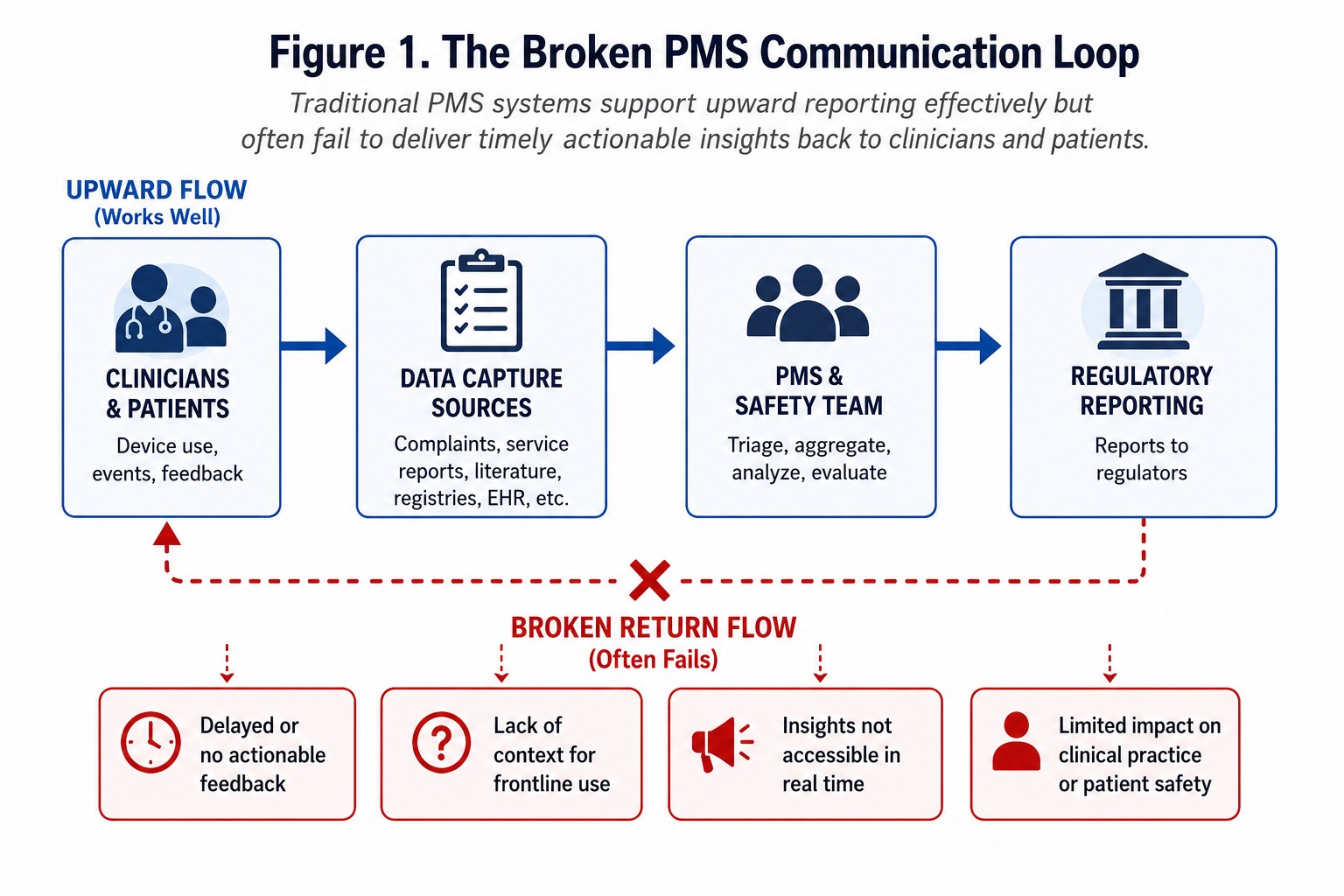
Today’s PMS systems are highly effective at upward communication: clinicians report issues, hospitals escalate concerns, manufacturers investigate, and regulators are notified.
However, the reverse flow—translating findings back into clinical action—is often fragmented, delayed, or unclear (Figure 1). Most PMS outputs are designed for regulatory traceability and documentation completeness rather than clinical usability.
 Clinicians rarely need lengthy aggregate reports or static trending summaries. What they need are clear thresholds for intervention, defined patient management pathways, and guidance on escalation or monitoring actions.
Clinicians rarely need lengthy aggregate reports or static trending summaries. What they need are clear thresholds for intervention, defined patient management pathways, and guidance on escalation or monitoring actions.
In practice, many PMS systems function as reporting engines rather than decision systems. Signal reviews may occur monthly or quarterly, but actionable feedback to clinicians can take substantially longer. By the time recommendations are implemented, opportunities for early intervention may already have passed.
This disconnect becomes especially problematic for complex devices involving software updates, connected systems, or rapidly evolving clinical workflows. In these environments, delays in translating post-market insights into operational action can increase both patient risk and organizational exposure.
The most mature organizations recognize that the value of PMS lies not in documenting issues after they occur, but in enabling earlier decisions capable of reducing downstream escalation.
The Real Challenge: Signal Detection and Prioritization
As PMS data sources continue to expand, organizations are increasingly facing signal fatigue. Modern PMS systems ingest information from complaints, service data, manufacturing deviations, literature reviews, and real-world evidence sources.
This creates an overwhelming number of potential signals including minor complaint fluctuations, isolated anomalies, and repetitive low-severity issues. In practice, meaningful risks can become buried within operational noise.
A statistically visible increase in cosmetic complaints, for example, may have little clinical significance, while a rare intermittent therapy interruption event may carry substantial patient risk despite low frequency.
Effective signal management therefore requires integration of statistical significance, clinical relevance, and consistency across data sources. Only when these dimensions align should a signal be considered actionable (Figure 2).
 One of the most common weaknesses in PMS systems is overreliance on frequency-based trending alone. High-volume issues are often prioritized because they are operationally visible, while low-frequency but clinically severe events may remain hidden. This creates a dangerous imbalance where organizations devote disproportionate attention to operational noise while underestimating emerging high-risk failure modes.
One of the most common weaknesses in PMS systems is overreliance on frequency-based trending alone. High-volume issues are often prioritized because they are operationally visible, while low-frequency but clinically severe events may remain hidden. This creates a dangerous imbalance where organizations devote disproportionate attention to operational noise while underestimating emerging high-risk failure modes.
Clinical context is therefore essential. Data alone cannot determine whether a signal materially changes patient risk, therapy delivery, or device effectiveness. Signal interpretation requires collaboration between quality, engineering, regulatory, and clinical functions to ensure that statistical trends are translated into meaningful risk evaluations.
As organizations continue integrating larger data sets, the ability to distinguish false signals from meaningful safety trends will increasingly become a defining competency of mature PMS systems.
Digital Enablers Are Transforming PMS
Organizations are increasingly investing in AI-enabled analytics, automated coding systems, integrated quality data platforms, and natural language processing tools.
These technologies are shifting PMS from a retrospective reporting function toward a more predictive capability. Advanced systems can identify subtle drift patterns, emerging failure modes, geographic clustering, and service trends preceding device failures before formal complaint thresholds are exceeded.
Natural language processing tools, for example, can analyze narrative complaint descriptions to identify recurring symptom patterns or device-use scenarios that may not be visible through traditional coding structures. Similarly, machine learning models can evaluate relationships between manufacturing variation, service trends, and complaint escalation to identify weak signals earlier in the product lifecycle.
Connected medical devices are also transforming PMS capabilities. Device telemetry, software logs, and real-time performance monitoring now provide organizations with significantly greater visibility into field performance than was historically possible.
However, technology alone does not solve the problem. Without defined escalation pathways, clear ownership, and structured prioritization frameworks, even sophisticated systems risk becoming repositories of unanalyzed data rather than operational decision-support tools.
Organizations therefore must align digital capabilities with governance structures capable of translating predictive insights into timely operational decisions.
Closing the Loop: From Detection to Action
The most mature PMS organizations are beginning to operate using a true closed-loop feedback model (Figure 3): Data Collection → Signal Detection → Risk Evaluation → Action → Design & Clinical Feedback.
 In practice, this means post-market insights continuously influence risk management files, CAPA activities, clinical guidance, product design improvements, and manufacturing controls.
In practice, this means post-market insights continuously influence risk management files, CAPA activities, clinical guidance, product design improvements, and manufacturing controls.
For example, a manufacturer may identify a recurring low-frequency software synchronization issue through complaint trending and telemetry analysis. Individually, complaints may appear isolated and remain below formal escalation thresholds. However, when integrated with service logs and clinical review, investigators may identify a pattern associated with temporary therapy interruption.
This can trigger enhanced monitoring criteria, targeted software updates, clinician communication, and design review activities before widespread field escalation occurs.
Importantly, closed-loop PMS models do not stop at investigation completion. The most effective systems continuously evaluate whether corrective actions successfully reduced risk, improved usability, or altered complaint behavior over time.
This creates a continuous learning cycle where post-market data directly informs future product development, process optimization, and risk management strategy. In many ways, mature PMS systems now function as organizational learning systems rather than simply compliance processes.
The organizations that operationalize this feedback loop effectively are often able to respond to emerging risks faster, reduce unnecessary escalations, and improve long-term product performance.
Regulatory Complexity Is Increasing—But Compliance Alone Is Not Enough
Global regulatory frameworks including FDA requirements, EU MDR, and UK MHRA PMS regulations have significantly expanded expectations around lifecycle monitoring, trending analyses, and risk documentation.¹⁻⁶
While these frameworks strengthen oversight, they also introduce administrative complexity and operational burden. Organizations now devote substantial effort toward maintaining PSURs, PMCF activities, vigilance reporting workflows, and regional documentation systems.
But regulatory compliance, while necessary, is not sufficient. The organizations that lead are those that treat PMS as a strategic capability—not simply a regulatory checkbox.
At the same time, many modern regulatory frameworks have undeniably improved traceability, lifecycle accountability, and transparency. Requirements surrounding Unique Device Identification (UDI), for example, have improved recall visibility and supply chain traceability across multiple regions.
The challenge is therefore not regulation itself. The challenge is ensuring that organizations maintain focus on patient impact and operational decision-making rather than becoming consumed by documentation activity alone.
As regulatory expectations continue to evolve, organizations will need PMS systems capable of balancing compliance obligations with real-world risk management effectiveness.
PMS Requires Organizational Change—Not Just Better Tools
One of the biggest barriers to effective PMS is organizational structure. In many companies, Quality owns complaint handling, Regulatory owns submissions, Engineering owns design changes, and Clinical teams interpret patient impact.
This fragmentation slows decision-making and weakens accountability.
High-performing organizations are increasingly adopting cross-functional signal review boards, shared risk governance models, integrated clinical review processes, and unified lifecycle dashboards to accelerate translation of PMS insights into operational action.
These organizations often establish recurring multidisciplinary reviews where engineering, quality, clinical, and regulatory teams evaluate emerging signals together rather than independently. Shared KPIs tied to signal response time, escalation quality, and complaint-to-design-change timelines help align organizational priorities across functions.
Leadership alignment is also critical. Without executive sponsorship, PMS initiatives often remain isolated within quality departments and fail to influence broader strategic decision-making.
As PMS systems become more predictive and data-intensive, organizations will increasingly require hybrid capabilities combining quality expertise, clinical interpretation, data analytics, and operational governance.
Practical Steps to Strengthen PMS Effectiveness
Organizations seeking to improve PMS effectiveness should focus on five priorities:
1. Prioritize signals based on clinical risk—not volume alone
2. Integrate complaints, service, manufacturing, and clinical evidence
3. Define structured escalation pathways for CAPAs and field actions
4. Embed clinical review early in signal evaluation
5. Continuously feed PMS insights back into risk management and product improvement activities
In addition, organizations should periodically evaluate whether PMS activities are generating measurable operational outcomes. Effective systems should demonstrate improvements in decision speed, risk visibility, complaint recurrence reduction, and field responsiveness over time.
PMS maturity should not be measured solely by documentation completeness or reporting frequency. It should also be measured by how effectively organizations identify meaningful risks and translate those insights into preventive action.
Conclusion: PMS as a Leadership Function
Post-market surveillance is no longer simply a back-end compliance activity.
It is a leadership function that directly impacts patient safety, clinical outcomes, product quality, and organizational trust.
The future of PMS will belong to organizations that can filter operational noise effectively, prioritize meaningful risks, and translate insights into action before issues escalate.
As connected devices, software-driven therapies, and real-world evidence continue reshaping MedTech, organizations capable of operationalizing post-market insights rapidly will gain a significant advantage in both safety and innovation.
Ultimately, the value of PMS is not determined by the volume of reports generated or the number of dashboards maintained. Its true value lies in whether organizations can identify emerging risks early enough to improve decisions, reduce escalation, and protect patients more effectively.
Data alone does not create safety. Decisions do.
Figure Captions
Figure 1. The Broken PMS Communication Loop
Traditional PMS systems support upward reporting effectively but often fail to deliver timely actionable insights back to clinicians and patients.
Figure 2. Signal Prioritization Framework
Effective PMS systems prioritize actionable signals using statistical significance, clinical relevance, and consistency across multiple data sources.
Figure 3. Closed-Loop PMS Operating Model
Mature PMS organizations integrate post-market data into continuous risk evaluation, CAPA activities, and product improvement processes.
References
- FDA 21 CFR Part 803 – Medical Device Reporting.
- FDA 21 CFR Part 820 – Quality System Regulation.
- Regulation (EU) 2017/745 on Medical Devices (EU MDR).
- ISO 14971:2019 Medical Devices — Application of Risk Management to Medical Devices.
- ISO 13485:2016 Medical Devices — Quality Management Systems.
- MDCG 2022-21 Guidance on Periodic Safety Update Reports (PSUR) under EU MDR.
The post From Compliance to Clinical Action: Fixing the Broken Loop in Post-Market Surveillance appeared first on MedTech Intelligence.


