HIT Consultant – Read More

Hospital leaders are navigating one of the most transformative periods in modern healthcare as organizations invest heavily in artificial intelligence, predictive analytics, and digital infrastructure. Yet one of the deadliest and most expensive forms of preventable harm inside hospitals receives far less strategic attention than it deserves: hospital-acquired pressure injuries.
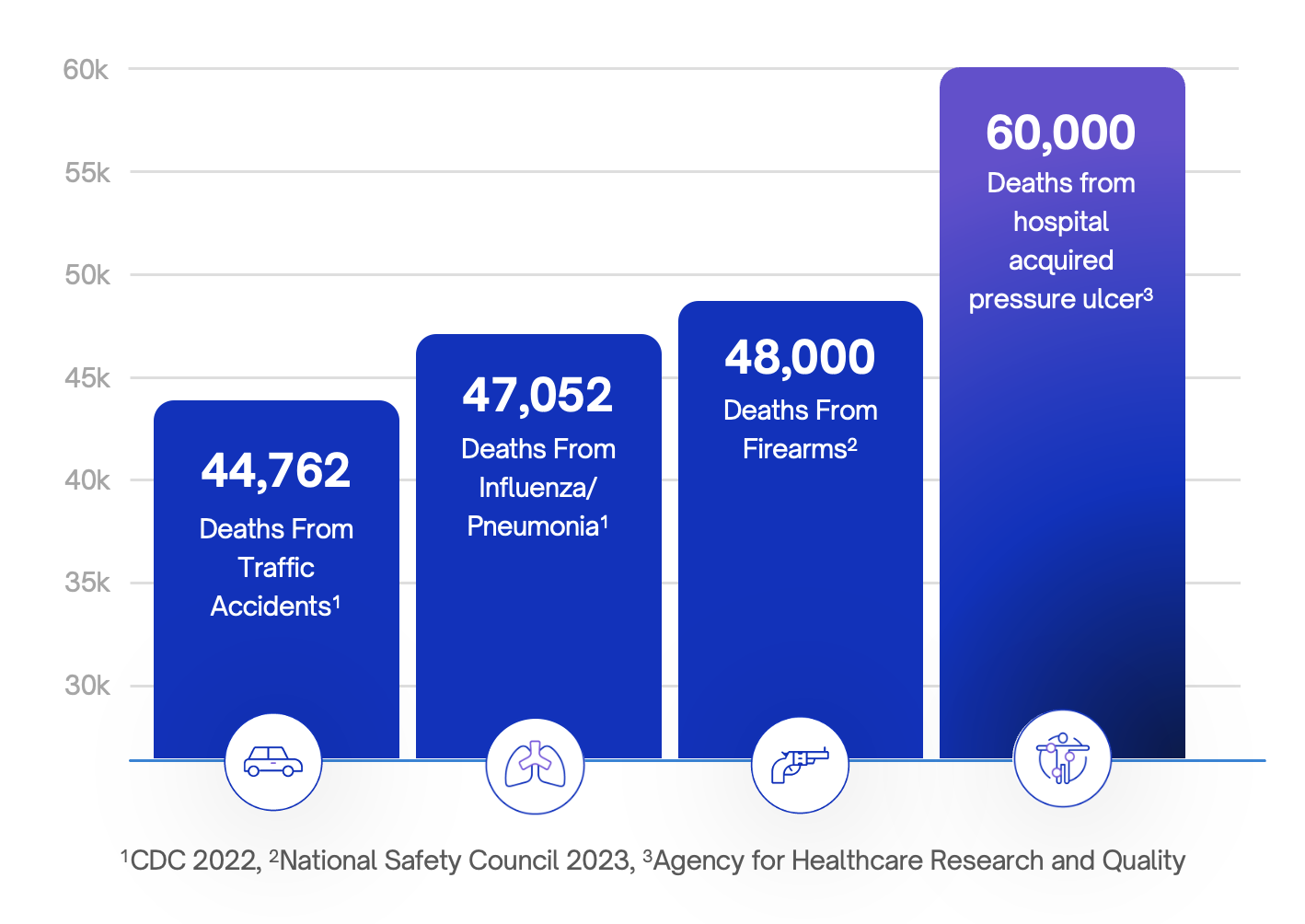
Pressure injuries contribute to an estimated 60,000 deaths annually in the United States, according to the Agency for Healthcare Research and Quality. That exceeds annual deaths from traffic accidents or influenza in many reporting periods. Nearly everyone will spend time in a hospital at some point in life, yet this risk remains largely invisible in public discourse and, too often, in executive strategy.
Through years of working alongside health systems and clinical teams, I have come to believe that pressure injury prevention represents a fundamental operational gap in modern healthcare delivery.
A Known Problem That Persists
Pressure injuries are not new. Clinical guidelines are well established, and prevention protocols have existed for decades. Hospitals understand risk factors, assessment tools, and recommended interventions.
Still, approximately 2.5 million patients develop pressure injuries in U.S. acute care settings each year. Critically ill patients face even higher exposure, with research showing that up to one in four ICU patients may develop a pressure injury during hospitalization.
The financial consequences are significant. Pressure injuries cost the healthcare system an estimated $26.8 billion annually. Individual cases can add between $20,900 and $151,700 in treatment costs. The National Pressure Injury Advisory Panel reports average legal settlements exceeding $200,000, contributing to roughly 17,000 lawsuits each year.
When outcomes remain unchanged despite widespread awareness, the issue is no longer clinical knowledge. It is operational execution.
The Gap Between Insight and Action
Healthcare has become exceptionally good at identifying risk. Electronic health records calculate scores automatically. Predictive analytics highlight vulnerable patients. Dashboards track quality indicators in real time. What these systems do not guarantee is that preventive care happens consistently at the bedside.
Repositioning and mobility, the core defenses against pressure injuries, depend on coordinated physical action delivered repeatedly throughout a patient’s stay. In many hospitals, execution relies almost entirely on nurses and frontline caregivers already managing heavy workloads and rising patient acuity.
Even highly skilled teams struggle to maintain perfect adherence when workflows compete for limited time and staffing. Technology can signal risk, but alerts alone do not move patients.
This creates a disconnect between digital intelligence and physical care delivery. Healthcare is measuring risk with precision while relying on fragile systems to address it.
A Workforce Challenge as Much as a Patient Safety Issue
Pressure injuries are often framed as patient outcomes, though they are equally tied to workforce sustainability.
Safe repositioning and mobility require physical effort. According to the Occupational Safety and Health Administration, musculoskeletal injuries linked to patient handling remain among the most common workplace injuries in healthcare. When caregivers are injured or fatigued, staffing shortages deepen and preventive care becomes harder to sustain.
In my conversations with nurse leaders, a consistent theme emerges. Care teams know what excellent prevention looks like. The difficulty lies in delivering it reliably within operational constraints.
Burnout grows when clinicians feel accountable for outcomes that depend on systems beyond their control.
Improving prevention therefore supports two priorities health systems are trying to solve simultaneously: protecting patients and stabilizing the workforce.
Why Prevention Requires Operational Ownership
Healthcare has successfully reduced harm in other areas by redesigning systems rather than relying solely on individual vigilance. Infection prevention improved through standardized workflows. Surgical safety advanced when structured processes reinforced consistency across teams.
Pressure injury prevention has not yet undergone the same operational evolution.
Hospital leadership teams should reconsider how prevention fits into enterprise strategy.
- First, mobility must be treated as a core clinical workflow supported by dedicated resources and accountability, not an additional task added to already full workloads.
- Second, measurement should focus on reliability of care delivery rather than documentation alone. Charting compliance does not always reflect whether preventive interventions occurred consistently.
- Third, technology investments should connect analytics directly to operational response. Predictive insights generate value only when systems exist to act on them dependably.
- Finally, leaders should evaluate prevention through a total-value perspective. Pressure injuries influence length of stay, reimbursement exposure, litigation risk, workforce injuries, and patient trust at the same time.
The Next Phase of Healthcare Transformation
Healthcare transformation is often discussed in terms of innovation and digital capability. Those advances are essential, but transformation also requires strengthening the reliability of fundamental care.
Patients enter hospitals assuming they will be protected from preventable harm during moments when they are least able to protect themselves. Pressure injuries challenge that expectation because they develop gradually, often unnoticed until damage becomes severe.
The industry does not lack awareness or clinical expertise. What it lacks is operational alignment that ensures prevention happens consistently for every patient.
If healthcare leaders want digital transformation to deliver its full promise, we must close the gap between what we know and what reliably occurs at the bedside. Pressure injury prevention offers a clear opportunity to do exactly that.
Until it becomes a strategic priority owned at the leadership level, one of the most lethal and costly complications in hospital care will remain a safety crisis hiding in plain sight.
About Eric Race, CEO of Atlas Mobility
Eric Race is the Founder and CEO of Atlas Mobility, a healthcare technology company headquartered in Miami, FL and San Francisco, CA. Atlas improves mobility, safety, and patient outcomes inside hospitals across the United States. Over the past decade, Eric has built Atlas from the ground up into a nationally deployed clinical operations company and FDA-registered medical device organization with approximately 400 employees nationwide. The company partners with leading health systems to reduce workplace injuries, standardize safe patient movement, and modernize frontline clinical operations.